For US Healthcare Professionals
I am a:
For US Healthcare Professionals
Full Prescribing Information



Patients saw clearer skin at Week 161,2
VOYAGE 1: Major secondary endpoints at Weeks 16, 24, and 48 (NRI)*
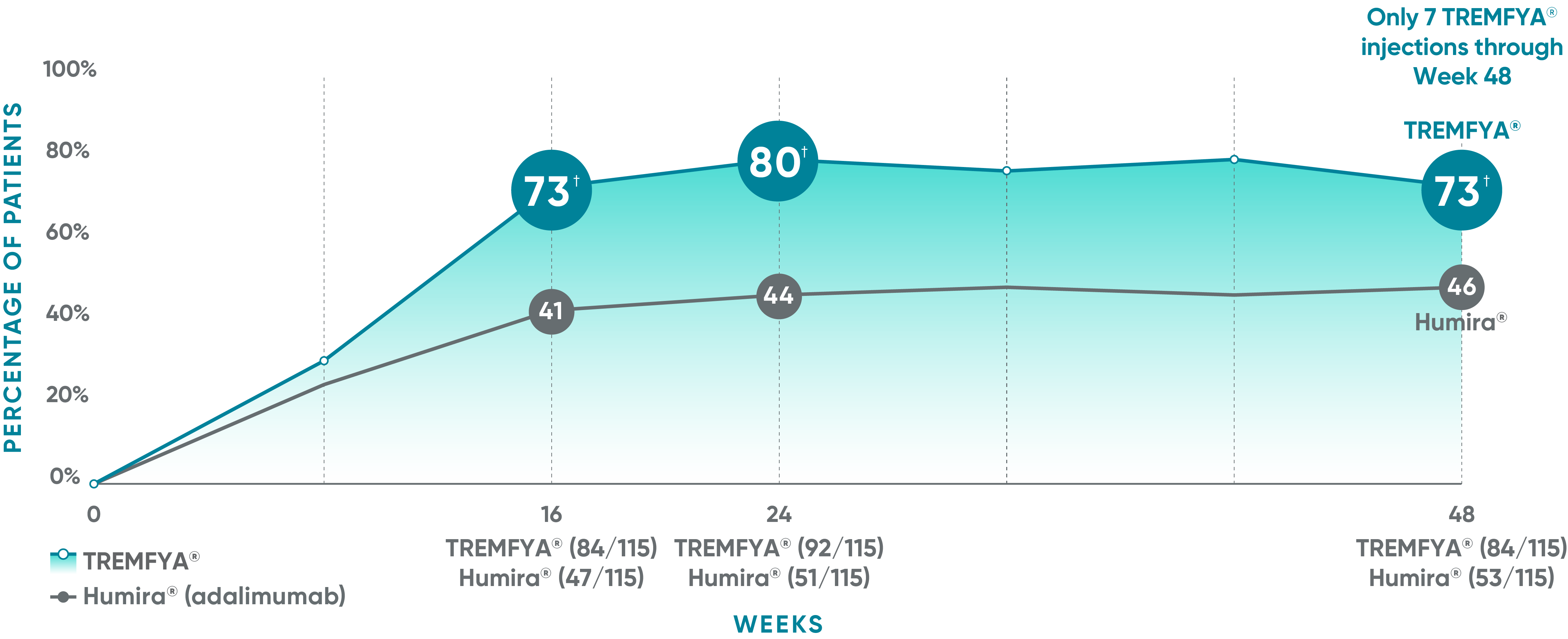


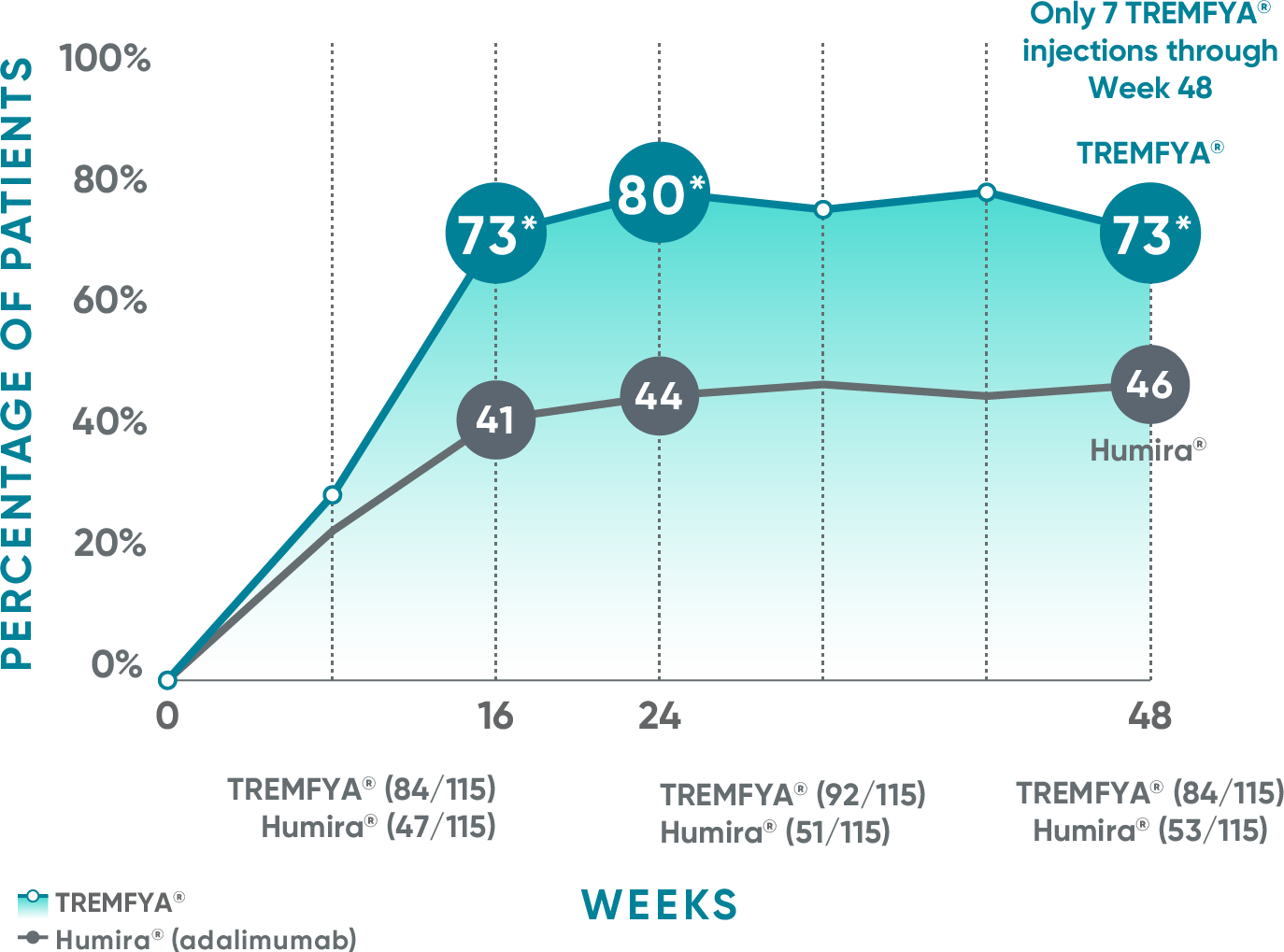
The same patients may not have responded at each time point.
VOYAGE co-primary endpoints at Week 16 (NRI)1,2:
VOYAGE 1—PASI 90: TREMFYA® 73% (241/329), placebo 3% (5/174) (P<0.001). IGA 0/1: TREMFYA® 85% (280/329), placebo 7% (12/174) (P<0.001). VOYAGE 2—PASI 90: TREMFYA® 70% (347/496), placebo 2% (6/248) (P<0.001). IGA 0/1: TREMFYA® 84% (417/496), placebo 8% (21/248) (P<0.001).
Psoriasis Symptoms and Signs Diary (Week 16): Greater improvements in symptoms of psoriasis (itch, pain, stinging, burning, and skin tightness).2
VOYAGE 2: Major secondary endpoint at Week 16 (NRI)1,2*†
- 64% (102/160) of patients receiving TREMFYA® achieved PASI 90 vs 42% (34/81) of patients receiving Humira®
VOYAGE 2: Major secondary endpoint at Week 24 (NRI)1,2*‡
- 71% (113/160) of patients receiving TREMFYA® achieved PASI 90 vs 51% (41/81) of patients receiving Humira®
*Results from North American sites only, which used US-licensed Humira®.
†P<0.001 vs Humira®.
‡P=0.003 vs Humira®.
Humira is a registered trademark of Abbvie Biotechnology Ltd. Corporation.
NRI=nonresponder imputation.
References: 1. Data on file. Janssen Biotech, Inc. 2. TREMFYA® (guselkumab) [Prescribing Information]. Horsham, PA: Janssen Biotech, Inc.
48% of patients were completely clear* at Week 481
VOYAGE 1: Prespecified exploratory endpoint at Weeks 24 and 48 (NRI)*†
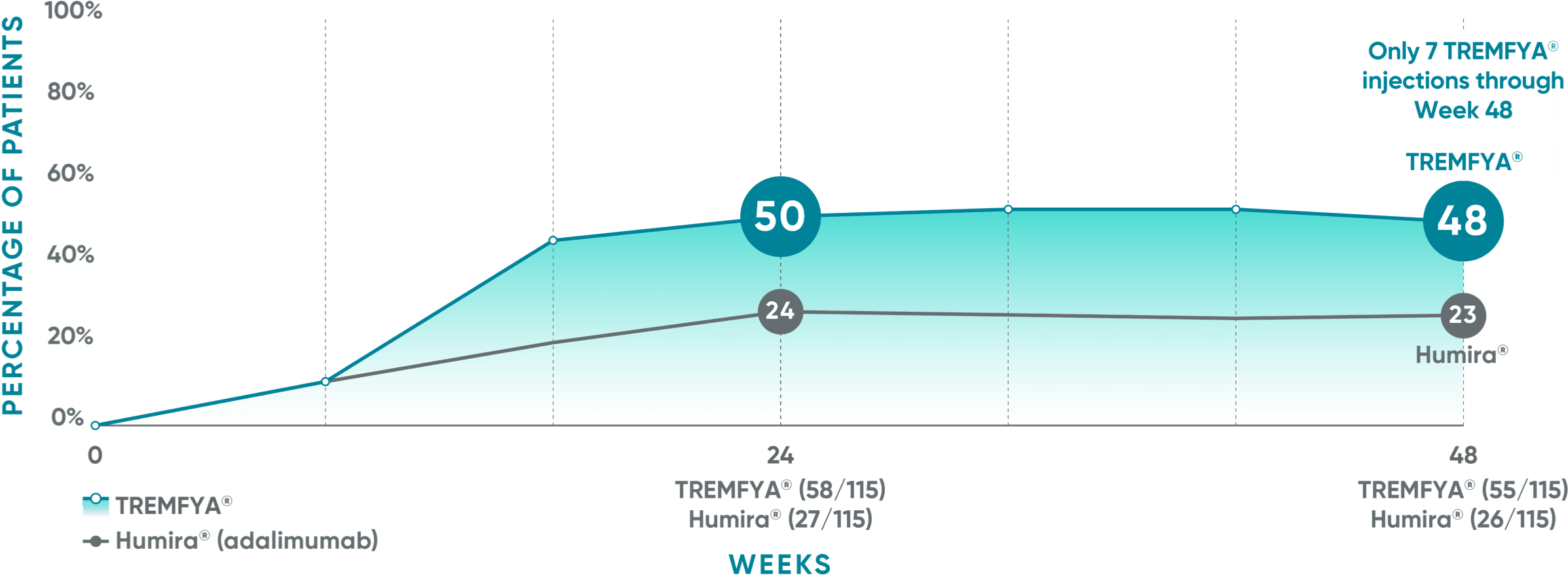
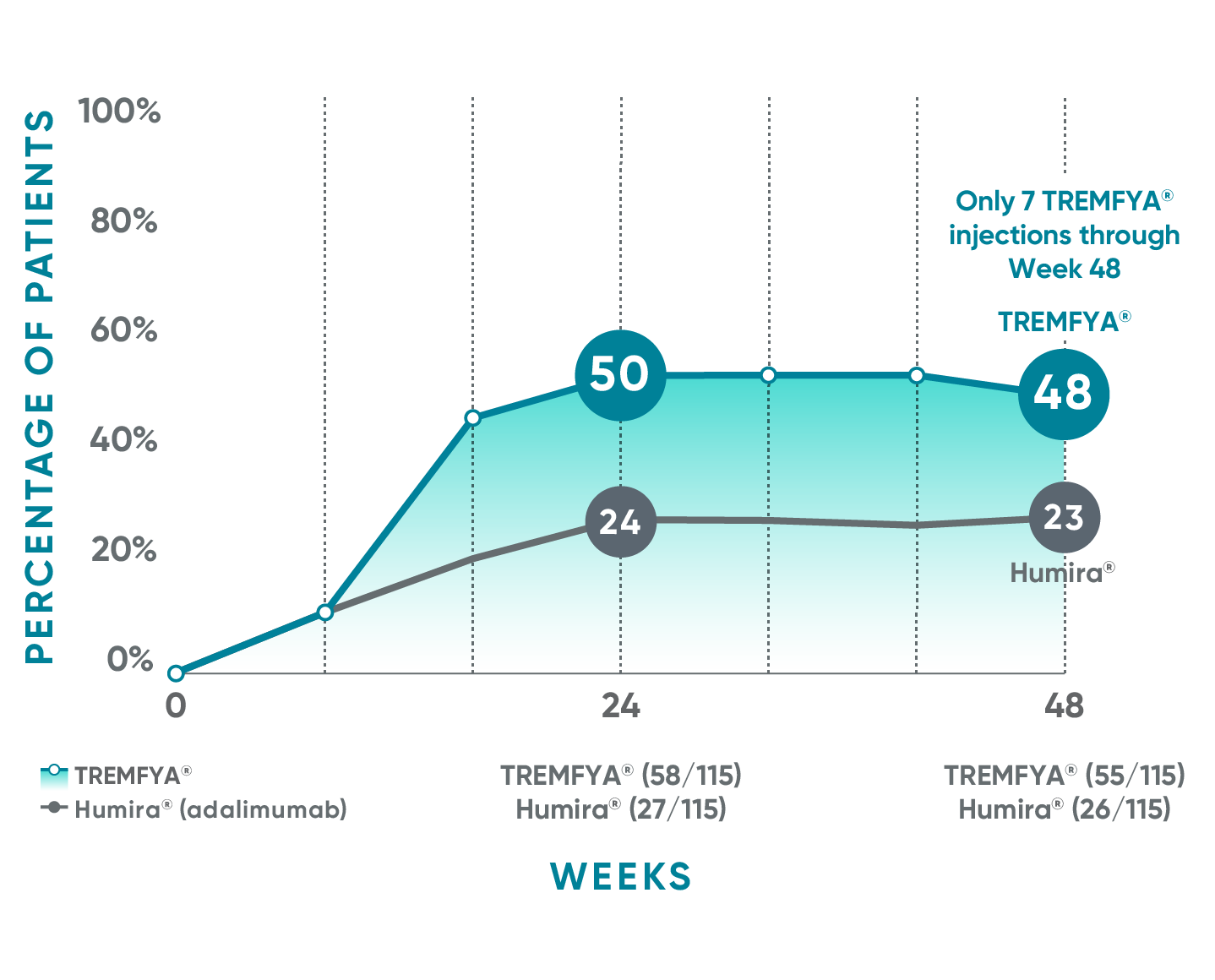
*PASI 100 was a prespecified exploratory endpoint that was not adjusted for multiplicity; P values were considered nominal.
The same patients may not have responded at each time point.
VOYAGE co-primary endpoints at Week 16 (NRI)1,2:
VOYAGE 1—PASI 90: TREMFYA® 73% (241/329), placebo 3% (5/174) (P<0.001). IGA 0/1: TREMFYA® 85% (280/329), placebo 7% (12/174) (P<0.001). VOYAGE 2—PASI 90: TREMFYA® 70% (347/496), placebo 2% (6/248) (P<0.001). IGA 0/1: TREMFYA® 84% (417/496), placebo 8% (21/248) (P<0.001).
Psoriasis Symptoms and Signs Diary (Week 16): Greater improvements in symptoms of psoriasis (itch, pain, stinging, burning, and skin tightness).2
†Results from North American sites only, which used US-licensed Humira®.
Humira is a registered trademark of Abbvie Biotechnology Ltd. Corporation.
NRI=nonresponder imputation; PASI 100=proportion of patients who achieved 100% reduction (or improvement) in PASI score from baseline.
References: 1. Data on file. Janssen Biotech, Inc. 2. TREMFYA® (guselkumab) [Prescribing Information]. Horsham, PA: Janssen Biotech, Inc.
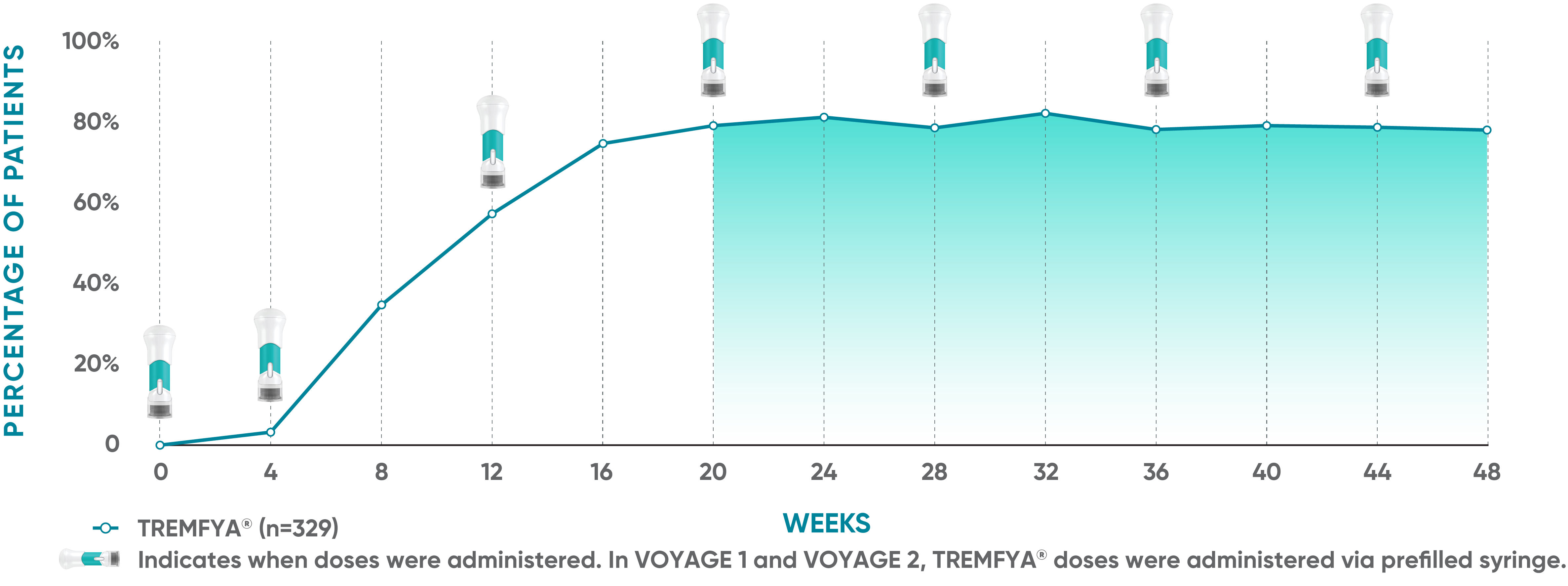
Consistent efficacy, dose to dose
VOYAGE 1: Prespecified secondary analysis—PASI 90 response rates
were evaluated between doses from Week 20 through Week 481,2*
-+

Data shown include patients randomized at Week 0 to the TREMFYA® arm.
The same patients may not have responded at each time point.
Placebo and active-comparator data are not shown in chart.
VOYAGE co-primary endpoints at Week 16 (NRI)2,3:
VOYAGE 1—PASI 90: TREMFYA® 73% (241/329), placebo 3% (5/174) (P<0.001). IGA 0/1: TREMFYA® 85% (280/329), placebo 7% (12/174) (P<0.001). VOYAGE 2—PASI 90: TREMFYA® 70% (347/496), placebo 2% (6/248) (P<0.001). IGA 0/1: TREMFYA® 84% (417/496), placebo 8% (21/248) (P<0.001).
Psoriasis Symptoms and Signs Diary (Week 16): Greater improvements in symptoms of psoriasis (itch, pain, stinging, burning, and skin tightness).3
VOYAGE 2: PASI 90 at Weeks 16 and 24 (major secondary endpoints, NRI)3†
- 64% (102/160) of patients receiving TREMFYA® achieved PASI 90 response at Week 16
- 71% (113/160) of patients receiving TREMFYA® achieved PASI 90 response at Week 24
*NRI methods were used for analysis.
†Results from North American sites only, which used a US-licensed active comparator. Active-comparator data not shown.
Dosing and administration
- 100 mg administered by subcutaneous injection at Week 0, Week 4, and every 8 weeks thereafter3
References: 1. Blauvelt A, Papp KA, Griffiths CEM, et al. Efficacy and safety of guselkumab, an anti-interleukin-23 monoclonal antibody, compared with adalimumab for the continuous treatment of patients with moderate to severe psoriasis: results from the phase III, double-blinded, placebo- and active comparator-controlled VOYAGE 1 trial. J Am Acad Dermatol. 2017;76(3):405-417. 2. Data on file. Janssen Biotech, Inc. 3. TREMFYA® (guselkumab) [Prescribing Information]. Horsham, PA: Janssen Biotech, Inc.
93% mean PASI improvement at Week 481
VOYAGE 1: Prespecified other secondary analysis—mean PASI improvement from baseline*

In the controlled period, mean PASI improvement was a prespecified other secondary analysis that was not adjusted for multiplicity; P values were considered nominal.
The same patients may not have responded at each time point.
VOYAGE co-primary endpoints at Week 16 (NRI)1,2:
VOYAGE 1—PASI 90: TREMFYA® 73% (241/329), placebo 3% (5/174) (P<0.001). IGA 0/1: TREMFYA® 85% (280/329), placebo 7% (12/174) (P<0.001). VOYAGE 2—PASI 90: TREMFYA® 70% (347/496), placebo 2% (6/248) (P<0.001). IGA 0/1: TREMFYA® 84% (417/496), placebo 8% (21/248) (P<0.001).
Psoriasis Symptoms and Signs Diary (Week 16): Greater improvements in symptoms of psoriasis (itch, pain, stinging, burning, and skin tightness).2
In VOYAGE 21
- Mean PASI improvement from baseline at Week 4 was 54% (n=496) with TREMFYA® vs 16% (n=248) with placebo
- Mean PASI improvement from baseline at Week 16 was 89% (n=496) with TREMFYA® vs 20% (n=248) with placebo
Treatment failure rules method: Patients who discontinued study agent due to lack of efficacy or an adverse event of worsening of psoriasis, or who started a protocol-prohibited medication, including conventional and biologic systemic therapy, phototherapy, and/or topical therapies for psoriasis, were considered treatment failures. Patients were considered to have no improvement (percent improvement=0) after meeting treatment failure criteria.
After treatment failure rules were applied, last observation carried forward was applied for any missing data.
*Mean PASI improvement is an assessment of the average percentage improvement from baseline in psoriatic signs of redness, thickness, scale, and body surface area of involvement.
References: 1. Data on file. Janssen Biotech, Inc. 2. TREMFYA® (guselkumab) [Prescribing Information]. Horsham, PA: Janssen Biotech, Inc.
Retreatment with TREMFYA® after withdrawal
and loss of ≥50% of PASI response at Week 281
VOYAGE 2: Prespecified exploratory endpoint—proportion of patients with ≥PASI 75 or ≥PASI 90 after retreatment
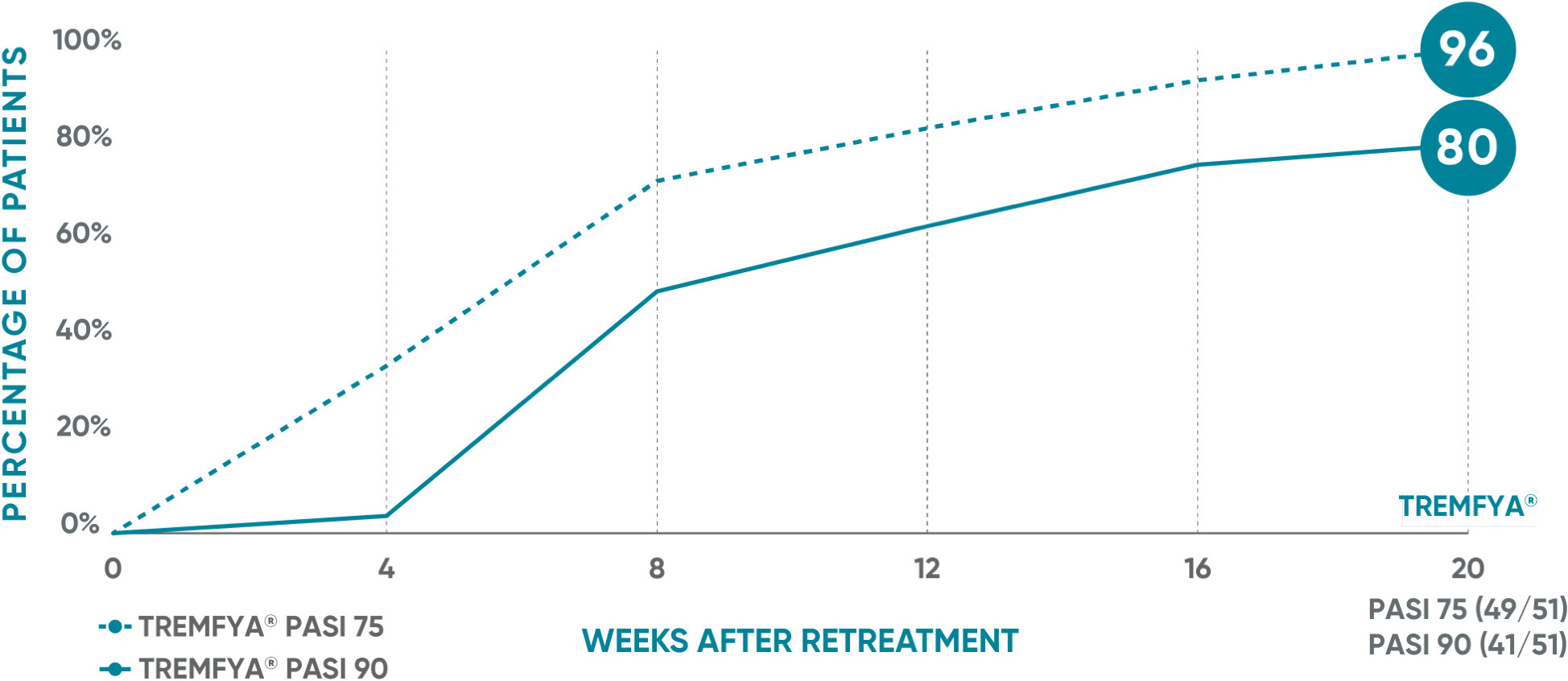
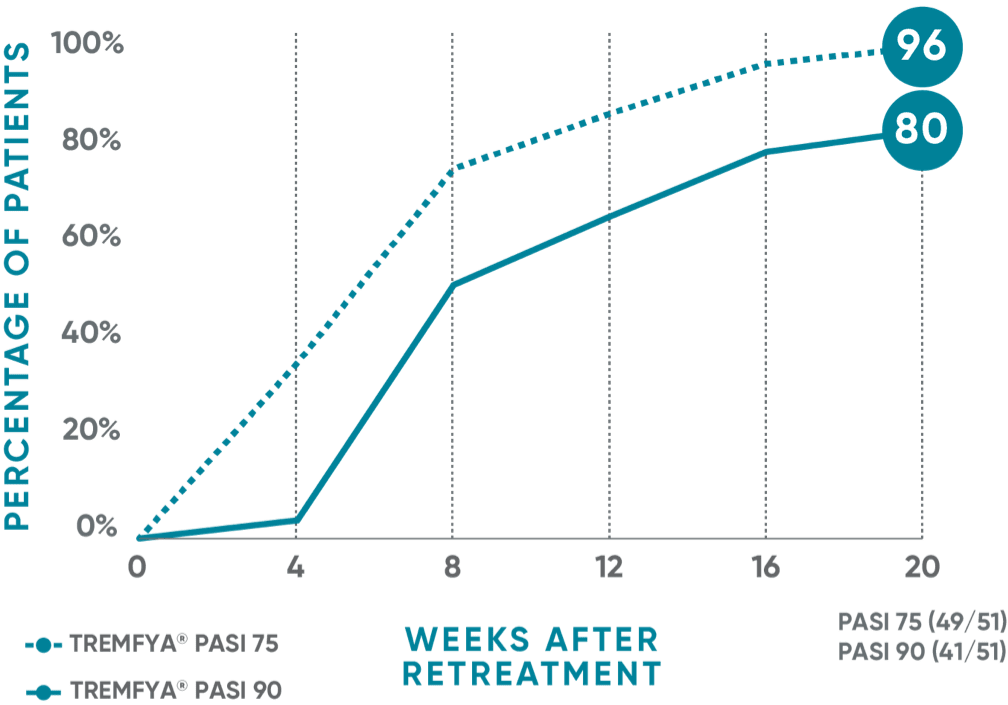
Limitations:
- The criterion for retreatment was patient-specific (ie, based on the patient’s baseline value and amount of improvement) and therefore includes a range of PASI scores
- The same patients may not have responded at each time point
VOYAGE co-primary endpoints at Week 16 (NRI)1,2:
VOYAGE 1—PASI 90: TREMFYA® 73% (241/329), placebo 3% (5/174) (P<0.001). IGA 0/1: TREMFYA® 85% (280/329), placebo 7% (12/174) (P<0.001). VOYAGE 2—PASI 90: TREMFYA® 70% (347/496), placebo 2% (6/248) (P<0.001). IGA 0/1: TREMFYA® 84% (417/496), placebo 8% (21/248) (P<0.001).
Psoriasis Symptoms and Signs Diary (Week 16): Greater improvements in symptoms of psoriasis (itch, pain, stinging, burning, and skin tightness).2
At Week 0 of VOYAGE 2, patients were randomized to TREMFYA® 100 mg at Weeks 0, 4, 12, and 20. At Week 28, PASI 90 responders were re-randomized to either continue TREMFYA® or to receive placebo. Upon loss of ≥50% of the improvement in PASI achieved at Week 28, patients in the placebo arm were re-treated with TREMFYA® and evaluated for PASI 75 and PASI 90 response. This analysis includes patients who lost ≥50% of the improvement in PASI achieved at Week 28 by Week 32, 36, 40, 44, 48, or 52.
Patients were re-treated with 100 mg, then 100 mg 4 weeks later, and then 100 mg every 8 weeks.
References: 1. Data on file. Janssen Biotech, Inc. 2. TREMFYA® (guselkumab) [Prescribing Information]. Horsham, PA: Janssen Biotech, Inc.
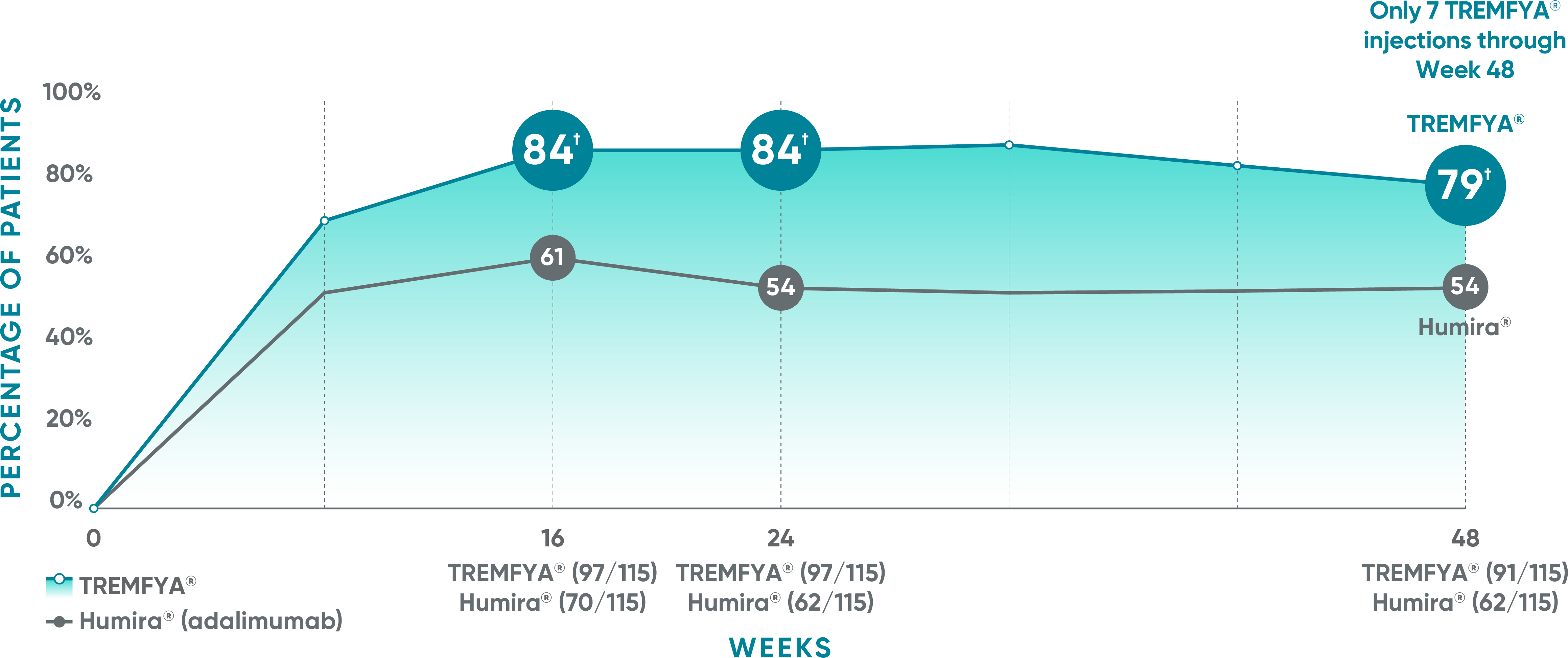
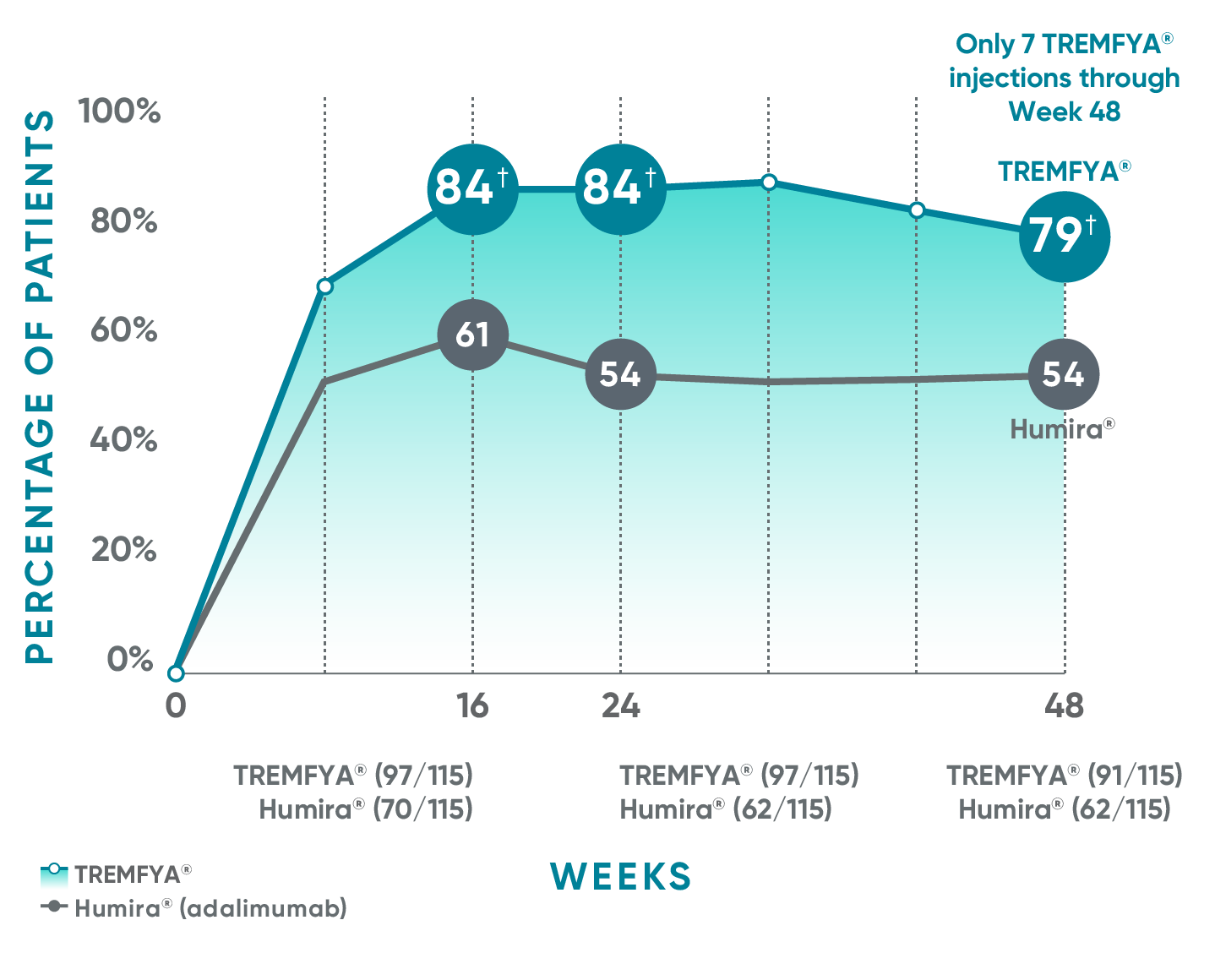
The majority of patients saw clearer skin with TREMFYA®1,2
VOYAGE 1: Major secondary endpoints at Weeks 16, 24, and 48 (NRI)*
The same patients may not have responded at each time point.
VOYAGE co-primary endpoints at Week 16 (NRI)1,2:
VOYAGE 1—PASI 90: TREMFYA® 73% (241/329), placebo 3% (5/174) (P<0.001). IGA 0/1: TREMFYA® 85% (280/329), placebo 7% (12/174) (P<0.001). VOYAGE 2—PASI 90: TREMFYA® 70% (347/496), placebo 2% (6/248) (P<0.001). IGA 0/1: TREMFYA® 84% (417/496), placebo 8% (21/248) (P<0.001).
Psoriasis Symptoms and Signs Diary (Week 16): Greater improvements in symptoms of psoriasis (itch, pain, stinging, burning, and skin tightness).2
VOYAGE 2: Major secondary endpoint at Week 16 (NRI)1,2*‡
- 74% (119/160) of patients receiving TREMFYA® achieved IGA 0/1 vs 62% (50/81) of patients receiving Humira®
VOYAGE 2: Major secondary endpoint at Week 24 (NRI)1,2*§
- 74% (119/160) of patients receiving TREMFYA® achieved IGA 0/1 vs 57% (46/81) of patients receiving Humira®
Humira is a registered trademark of Abbvie Biotechnology Ltd. Corporation.
Nonresponder imputation (NRI) methods were used for analysis.
*Results from North American sites only, which used US-licensed Humira®.
†P<0.001 vs Humira®.
‡P<0.027 vs Humira®.
§P=0.005 vs Humira®.
References: 1. Data on file. Janssen Biotech, Inc. 2. TREMFYA® (guselkumab) [Prescribing Information]. Horsham, PA: Janssen Biotech, Inc.
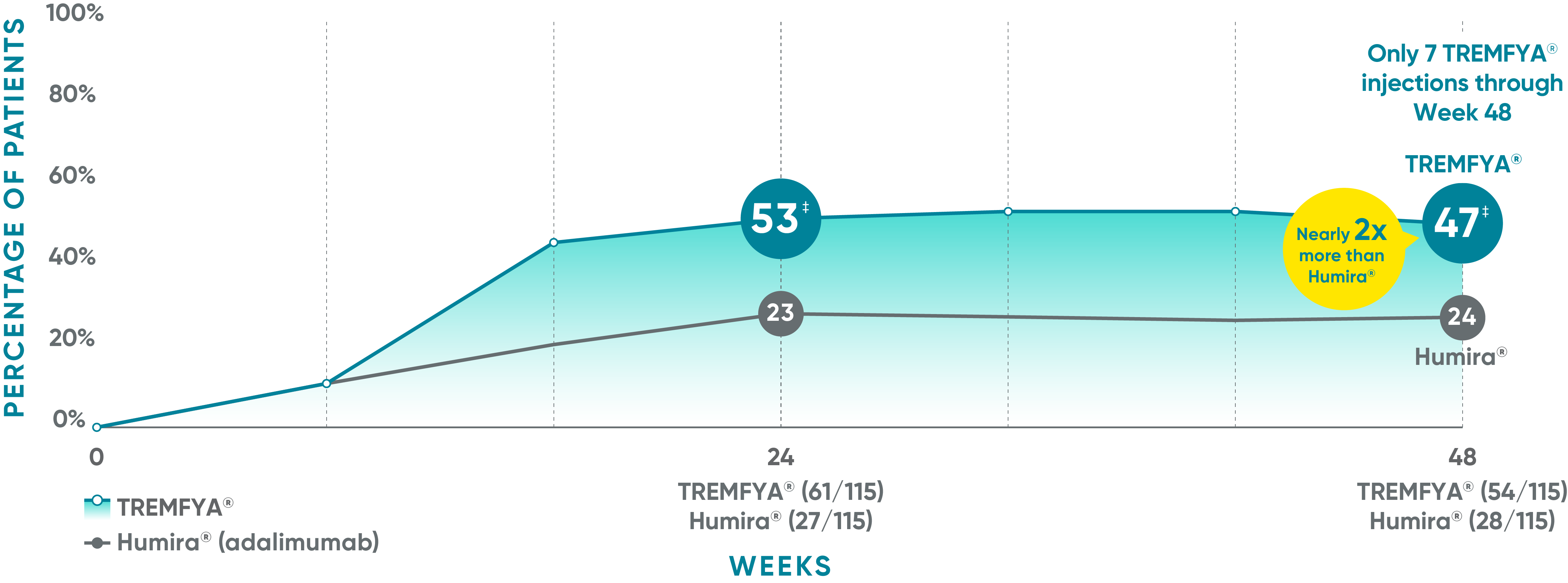
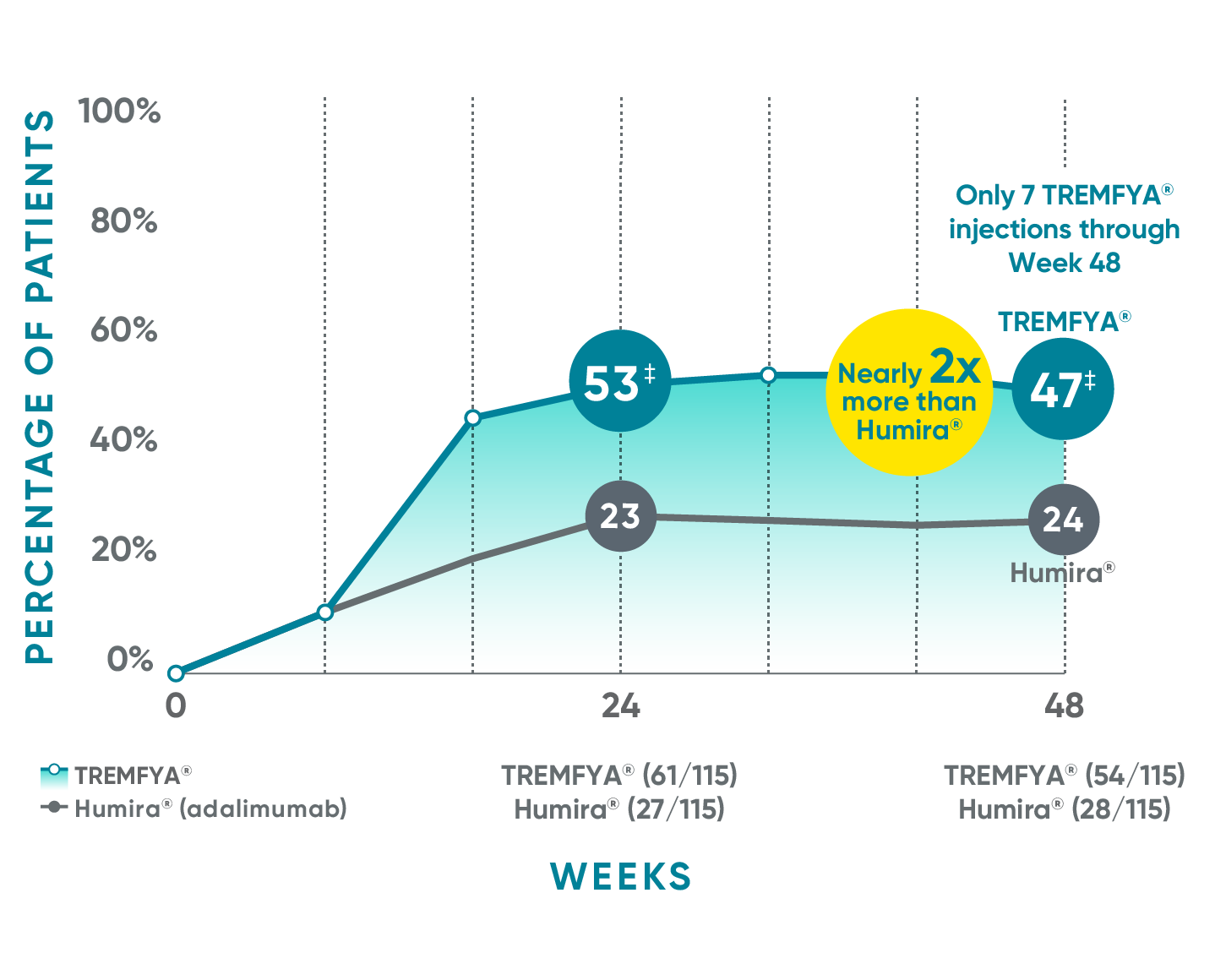
More than half of patients were completely clear at Week 241,2
VOYAGE 1: Major secondary endpoints at Weeks 24 and 48*†
The same patients may not have responded at each time point.
VOYAGE co-primary endpoints at Week 16 (NRI)1,2:
VOYAGE 1—PASI 90: TREMFYA® 73% (241/329), placebo 3% (5/174) (P<0.001). IGA 0/1: TREMFYA® 85% (280/329), placebo 7% (12/174) (P<0.001). VOYAGE 2—PASI 90: TREMFYA® 70% (347/496), placebo 2% (6/248) (P<0.001). IGA 0/1: TREMFYA® 84% (417/496), placebo 8% (21/248) (P<0.001).
Psoriasis Symptoms and Signs Diary (Week 16): Greater improvements in symptoms of psoriasis (itch, pain, stinging, burning, and skin tightness).2
VOYAGE 2: Major secondary endpoint at Week 241,2*†
- 48% (76/160) of patients receiving TREMFYA® achieved IGA 0 compared with 28% (23/81) of patients receiving Humira®
(P =0.005)
*NRI methods were used for analysis.
†Results from North American sites only, which used a US-licensed active comparator.
†P<0.001 vs Humira®.
References: 1. Data on file. Janssen Biotech, Inc. 2. TREMFYA® (guselkumab) [Prescribing Information]. Horsham, PA: Janssen Biotech, Inc.